What are fibroids?
Fibroids are non – cancerous or benign growths arising out of the uterus or its musculature
And are usually restricted to female reproductive organs.
What are the different types of fibroids?
The type of fibroid a woman develops depends on its location.
Intramural fibroids
Intramural fibroids are the most common type of fibroid, which appear within the muscular wall of the uterus. Intramural fibroids may grow larger and can stretch your womb.
Subserosal fibroids
Subserosal fibroids form on the outside of your uterus, which is called the serosa. They may grow large enough to make your womb appear bigger on one side than the other.
Pedunculated fibroids
Subserosal tumors can develop a long stem and a slender base that supports the tumor. When they do, they’re known as pedunculated fibroids.
Submucosal fibroids
These types of tumors develop in the inner and middle muscle layer, or endometrium, of your uterus. Submucosal tumors aren’t as common as the other types.
What causes fibroids?
It’s unclear why fibroids develop, but several factors may influence their formation.
Hormones
Estrogen and progesterone are the hormones produced by the ovaries. They cause the uterine lining to regenerate during each menstrual cycle and may stimulate the growth of fibroids.
Family history
Fibroids may run in the family. If your mother, sister, or grandmother has a history of this condition, you may develop it as well.
Pregnancy
Pregnancy increases the production of estrogen and progesterone in your body. Fibroids may develop and grow rapidly during pregnancy.
What are the symptoms of fibroids?
Your symptoms will depend on the number of tumors you have as well as their location and size. For instance, submucosal fibroids may cause heavy menstrual bleeding and trouble in conceiving.
If your tumor is very small or you’re going through menopause, you may not have any symptoms. Fibroids may shrink during and after menopause. This is because women undergoing menopause are experiencing a drop in their levels of estrogen and progesterone, hormones that stimulate fibroid growth.
- Symptoms of fibroids may include:
- Heavy bleeding between and during periods that includes blood clots
- pain in the pelvis and backache
- increased menstrual cramping
- Increased urination
- Pain during intercourse
- menstruation that lasts longer than usual
- Fullness in the lower abdomen
How to diagnose fibroids?
Fibroids are diagnosed using Ultrasound and MRI. Transvaginal ultrasound is the most accurate method of locating and assessing the fibroid.
How to treat fibroids?
- medical method – drugs like mifepristone, GnRH analogs are still experimental.
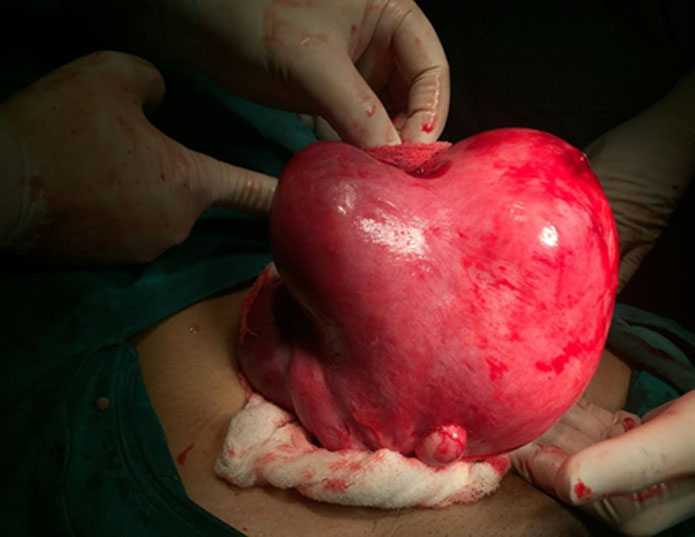
- surgery – Myomectomy or removal of fibroids. This is done laparoscopically in advanced setups.
- hysterectomy or removal of the uterus.
Fibroids Management by Laparoscopy in Greater Kailash
Laparoscopy is being done in all the leading hospitals in South Delhi. Dr. Ruchi Tandon has received extensive training in laparoscopy from the best hospitals in Delhi and Mumbai, such as moolchand hospital, leelavati hospital. Dr. Ruchi Tandon is one of the best gynecologists, based in greater Kailash and doing all sorts of daycare and operative laparoscopic procedures. Infertility surgeries, Myomectomy, hysterectomy, Hysteroscopy are some of the procedures to name a few. she is doing these procedures at Max smart super specialty hospital, Saket, Apollo Cradle Royale, and Apollo Spectra. In lieu of her experience and contribution to this field, she was conferred with the “best budding endoscopic surgeon “(National) award by the Economic Times at a grand event on 4th October, recently in Delhi.