Endometriosis causes chocolate cysts. Endometrial tissue lines the uterus, and endometriosis causes this tissue to grow outside the uterus as well.
Endometrial tissue can attach to the ovaries, fallopian tubes, and nearby organs, such as the bladder. This can cause painful, heavy periods, and it can also damage the organs that it affects.
Doctors divide endometriosis into stages, according to how far the endometrial tissue has spread to other areas of the body. Stages 3 and 4 are the most severe, and they are the most likely to cause endometriomas.
If a person with endometriosis does not receive treatment, it can grow more severe, and chocolate cysts may develop.
Chocolate cysts are sacs containing old blood. They attach to the ovaries and can affect ovarian function. In some cases, chocolate cysts can stop the ovaries from working and so prevent pregnancy.
Doctors do not know what causes endometriosis. Most research suggests that estrogen plays a key role,researchers are unsure why the hormone causes the condition in some people and not others.
Risk factors for endometriosis and chocolate cysts can include:
• Genetics: People with a family history of endometriosis are more likely to get the condition.
• Retrograde menstrual flow: This happens when period blood travels in the reverse direction, going up the fallopian tubes instead of out of the vagina.
• Immune disorders: Certain immune system issues, especially autoimmune disorders, may cause endometriosis.
• Injuries: Damage to the uterus or surrounding structures correlate with an increased risk of endometriosis. These injuries can occur, for example, during cesarean delivery.
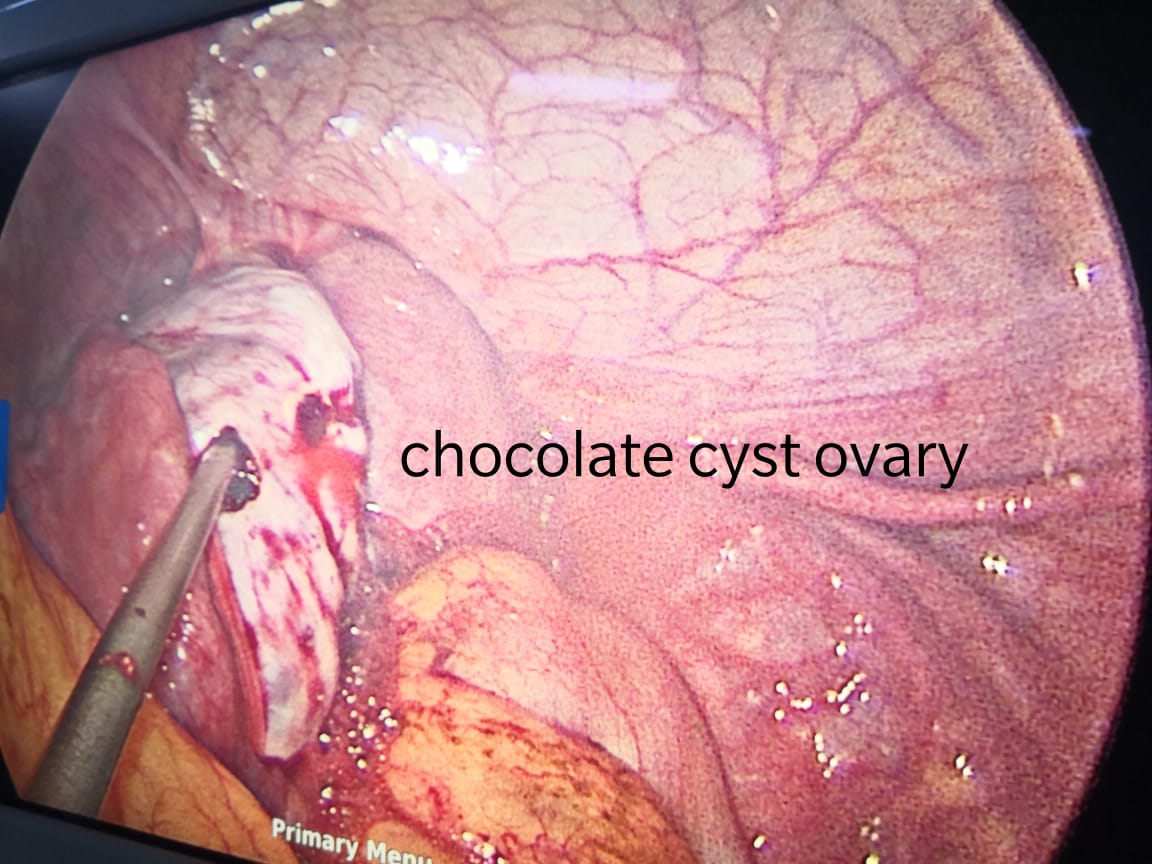
Chocolate cysts are noncancerous, fluid-filled cysts that typically form deep within the ovaries. They get their name from their brown, tar-like appearance, looking something like melted chocolate. They’re also called ovarian endometriomas.
The color comes from old menstrual blood and tissue that fills the cavity of the cyst. A chocolate cyst can affect one or both ovaries, and may occur in multiples or singularly.
Chocolate cysts occur in 20 to 40 percent of women who have endometriosis, estimates the Endometriosis Foundation of America.
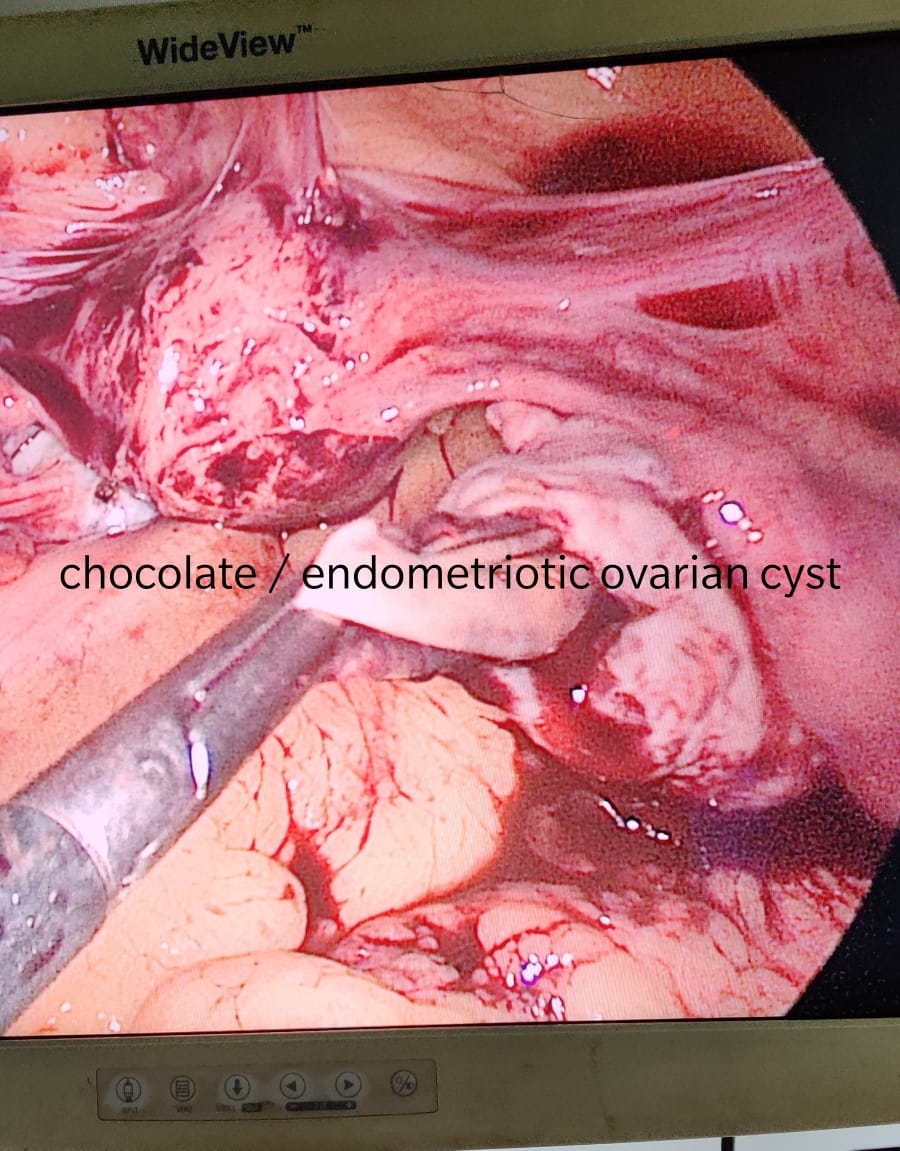
Endometriosis is a common disorder in which the lining of the uterus, known as the endometrium, grows outside the uterus and onto the ovaries, fallopian tubes, and other areas of the reproductive tract. The overgrowth of this lining causes severe pain and sometimes infertility.
Chocolate cysts are a subgroup of endometriosis. They’re often associated with more severe forms of the disorder.
What are the symptoms?
Chocolate cysts may cause symptoms in some women. Other women may not experience any symptoms.
The size of the cyst also doesn’t necessarily affect the severity or presence of symptoms. This means a woman with a small cyst may experience symptoms, while someone with a large one may not. Cysts can range from 2 to 20 centimeters (cm) in size.
When symptoms do occur, they’re similar to those of endometriosis. They can include:
• painful, crampy periods
• pelvic pain not related to your menstrual cycle
• irregular periods
• pain during sex
• infertility for some women
If a chocolate cyst ruptures, it can cause severe, sudden abdominal pain on the side of the body where the cyst is located. A ruptured cyst can be a medical emergency. Seek immediate medical attention if you suspect you have a ruptured cyst.
How are chocolate cysts diagnosed?
Your doctor may order a pelvic ultrasound if:
• they feel a cyst during a pelvic exam
• they suspect you have endometriosis based on your symptoms
• you’re experiencing unexplained infertility
An ultrasound can identify if a cyst is present. But it can’t necessarily determine what type of cyst it is.
To definitively diagnose a chocolate cyst, your doctor will extract fluid and debris from inside the cyst. This is usually done with a needle biopsy.
During a needle biopsy, your Gynecologist will use ultrasound to help them insert a needle through the vagina into the ovarian cyst. The extracted fluid is then examined under a microscope. Your Gynecologist can diagnose the type of cyst using the results from the needle biopsy.
Dr. Ruchi Tandon is a Gynecologist practicing in leading hospitals in South Delhi, namely Max and Apollo hospitals, she has over 13 years experience in handling endometriosis and all kinds of ovarian cysts.