Spontaneous pregnancy loss is a surprisingly common occurrence, with approximately 15% of all clinically recognized pregnancies resulting in pregnancy failure. Recurrent pregnancy loss (RPL) has been inconsistently defined. When defined as 3 consecutive pregnancy losses prior to 20 weeks from the last menstrual period, it affects approximately 1% to 2% of women. This review highlights the current understanding of the various etiologies implicated in RPL, including factors known to be causative, as well as those implicated as possible causative agents. The appropriate diagnostic evaluation, therapy, and prognosis are also addressed.
Spontaneous pregnancy loss is a surprisingly common occurrence. Whereas approximately 15% of all clinically recognized pregnancies result in spontaneous loss, there are many more pregnancies that fail prior to being clinically recognized. Only 30% of all conceptions result in a live birth.
Spontaneous pregnancy loss can be physically and emotionally taxing for couples, especially when faced with recurrent losses. Recurrent pregnancy loss (RPL), also referred to as recurrent miscarriage or habitual abortion, is historically defined as 3 consecutive pregnancy losses prior to 20 weeks from the last menstrual period. Based on the incidence of sporadic pregnancy loss, the incidence of recurrent pregnancy loss should be approximately 1 in 300 pregnancies. However, epidemiologic studies have revealed that 1% to 2% of women experience recurrent pregnancy loss.
Defining RPL as a clinical entity requiring diagnostic testing and therapeutic intervention rests on knowledge of the elevation of risk for subsequent fetal loss and the probability of finding a treatable etiology for the disorder. Although no reliable published data have estimated the probability of finding an etiology for RPL in a population with 2 versus 3 or more miscarriages, the best available data suggest that the risk of miscarriage in subsequent pregnancies is 30% after 2 losses, compared with 33% after 3 losses among patients without a history of a live birth. This strongly suggests a role for evaluation after just 2 losses in patients with no prior live births. An earlier evaluation may be further indicated if fetal cardiac activity was identified prior to a loss, the woman is older than 35 years, or the couple has had difficulty in conceiving.
The high baseline rate of spontaneous isolated and recurrent pregnancy losses in the general population, the lack of consistent definition for RPL, limited access to tissues allowing study of the disorder, and the remarkably good prognosis for live birth among patients with RPL combine to frustrate aims at diagnostic and therapeutic recommendations. At present, there exist a small number of accepted etiologies for RPL.These include parental chromosomal abnormalities, untreated hypothyroidism, uncontrolled diabetes mellitus, certain uterine anatomic abnormalities, and antiphospholipid antibody syndrome (APS). Other probable or possible etiologies include additional endocrine disorders, heritable and/or acquired thrombophilias, immunologic abnormalities, infections, and environmental factors. After evaluation for these causes , approximately half of all cases will remain unexplained.
Genetic Etiologies
Approximately 2% to 4% of RPL is associated with a parental balanced structural chromosome rearrangement, most commonly balanced reciprocal or Robertsonian translocations. Additional structural abnormalities associated with RPL include chromosomal inversions, insertions, and mosaicism. Single gene defects, such as those associated with cystic fibrosis or sickle cell anemia, are seldom associated with RPL.
Appropriate evaluation of RPL should include parental karyotyping. Genetic counseling is indicated in all cases of RPL associated with parental chromosomal abnormalities. Depending on the particular diagnosis, directed therapy may include in vitro fertilization with preimplantation genetic diagnosis. The use of donor gametes may be suggested in cases involving genetic anomalies that always result in embryonic aneuploidy (ie, Robertsonian translocations involving homologous chromosomes).
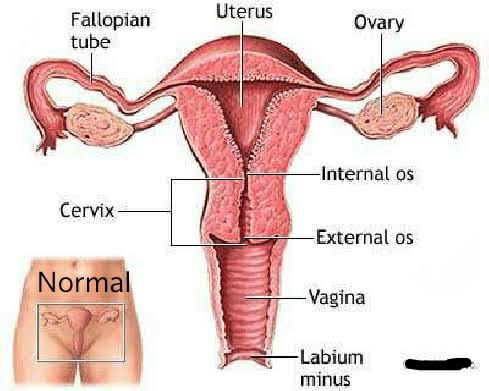
Anatomic Etiologies
Anatomic abnormalities account for 10% to 15% of cases of RPL and are generally thought to cause miscarriage by interrupting the vasculature of the endometrium, prompting abnormal and inadequate placentation. Thus, those abnormalities that might interrupt the vascular supply of the endometrium are thought to be potential causes of RPL. These include congenital uterine anomalies, intrauterine adhesions, and uterine fibroids or polyps. Although more readily associated with second trimester losses or preterm labor, congenital uterine anomalies also play a part in RPL.
The uterine septum is the congenital uterine anomaly most closely linked to RPL, with as much as a 76% risk of spontaneous pregnancy loss among affected patients. Other Müllerian anomalies, including unicornuate, didelphic, and bicornuate uteri have been associated with smaller increases in the risk for RPL. The role of the arcuate uterus in causing RPL is unclear. The presence of intrauterine adhesions, sometimes associated with Asherman syndrome, may significantly impact placentation and result in early pregnancy loss.
Intramural fibroids larger than 5 cm, as well as submucosal fibroids of any size, can cause RPL. Although congenital anomalies caused by prenatal exposure to diethylstilbestrol are clearly linked to RPL, this is becoming less clinically relevant as most affected patients move beyond their reproductive years.
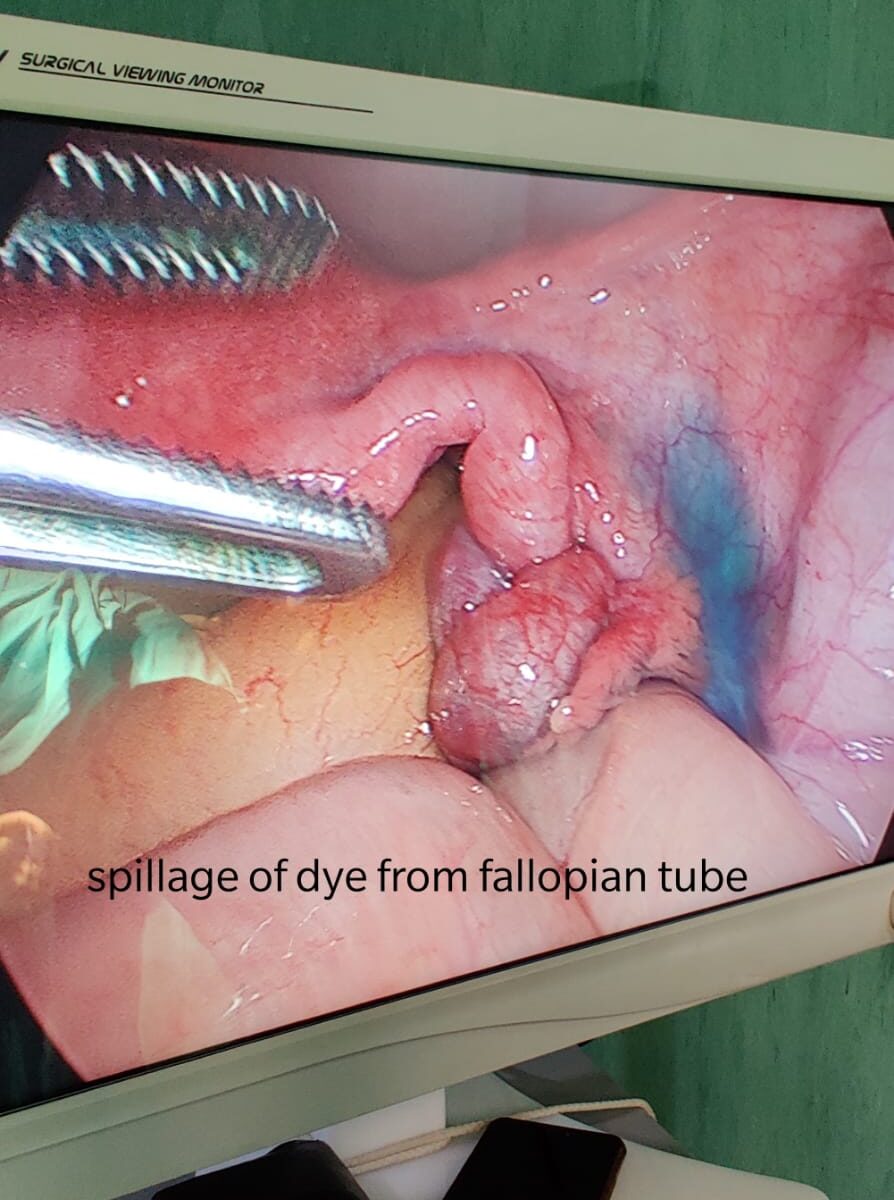
Diagnostic evaluation for uterine anatomic anomalies should include office hysteroscopy or hysterosalpingography (HSG). Hysteroscopic resection of intrauterine adhesions and intrauterine septa are indicated if these abnormalities are identified. Patients undergoing successful hysteroscopic septum resection seem to enjoy near normal pregnancy outcomes, with term delivery rates of approximately 75% and live birth rates approximating 85%.Myomectomy should be considered in cases of submucosal fibroids or any type fibroids larger than 5 cm. Resection has been shown to significantly improve live birth rates from 57% to 93%.Myomectomy can be performed via open laparotomy, laparoscopy, or hysteroscopy.
Dr. Ruchi Tandon is a reputed Gynecologist practicing in leading hospitals in South Delhi namely Max and Apollo hospitals with over 14 years of experience in handling all kinds of Gynecological conditions including recurrent abortions.