Menopause occurs when a woman has not had her menstrual period for a year. This occurrence is the result of a natural decline in hormones that a woman will experience usually in her 40s or 50s.
When a woman has gone through menopause, she normally does not expect to have any further bleeding. However, women may sometimes experience additional vaginal bleeding. If she has gone through menopause, doctors consider the bleeding abnormal, and a woman should contact her Gynecologist.
Examples of bleeding symptoms that could indicate that she needs to call her doctor include bleeding after sex or bleeding that is very heavy and more than “spotting.” Most commonly, the bleeding is unrelated to an issue with menstruation and may be due to another cause that should be identified.
Postmenopausal bleeding can be due to a number of causes. Examples of some of the most common causes include:
• Endometrial atrophy: When the hormone estrogen stops being produced due to menopause, a woman’s endometrial lining may start to become thinner. As a result, the lining of the endometrium may be more likely to bleed.
• Endometrial hyperplasia: This condition causes the uterine lining to become thicker instead of thinner, giving rise to heavy or irregular bleeding. The cause of this condition is most commonly excess estrogen without the hormone progesterone to offset it. Endometrial hyperplasia can sometimes lead to the development of endometrial cancer.
• Endometrial cancer: This is cancer of the endometrial lining. An estimated 10 percent of postmenopausal women with uterine bleeding experience the bleeding due to endometrial cancer.
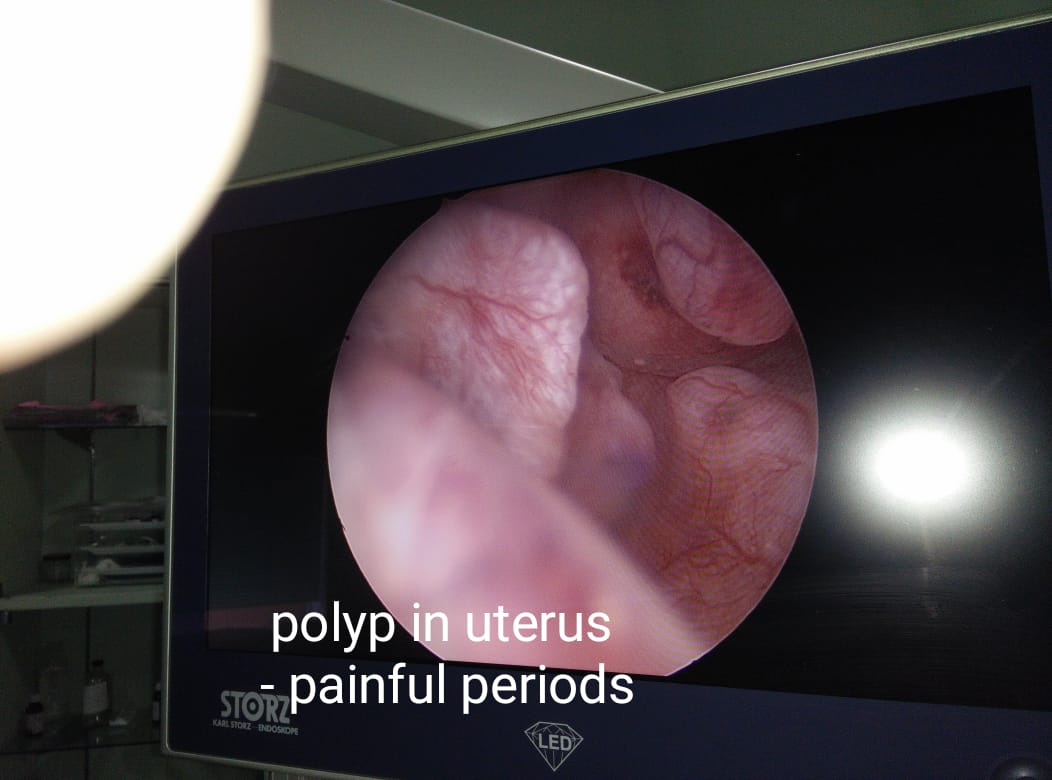
• Polyps: Polyps are growths that can develop on the lining of the uterus. They are usually noncancerous but can cause unusual or heavy bleeding. Polyps can sometimes grow inside the cervical canal. When this occurs, a woman may experience bleeding when she has sex.
Other potential, but less likely, causes of postmenopausal bleeding include:
• clotting problems
• infection of the uterine lining, which is known as endometritis
• trauma to the pelvis
• bleeding from the urinary tract
• thyroid disorders
Hormone medications, such as tamoxifen, may also cause postmenopausal bleeding as a side effect. Many women will experience breakthrough bleeding as a result of taking hormone replacement therapy in the first 6 months.
Regardless of the potential underlying cause, it is important that a woman sees her doctor when she has vaginal bleeding.
Diagnosis
A Gynecologist will start an exam for postmenopausal bleeding by asking the woman about the symptoms she may be experiencing. A Gynecologist will likely ask:
• when she first noticed her symptoms
• how much she bleeds
• if she has any family history of postmenopausal bleeding
Depending upon a woman’s symptoms, a doctor may recommend one or more of a number of tests.
Examples of tests used to diagnose the cause of postmenopausal bleeding include:
Examples of tests used to diagnose the cause of postmenopausal bleeding include:
• Dilation and curettage (D&C): This procedure involves dilating or widening the cervix to obtain a larger tissue sample. It also involves using a special tool called a hysteroscope to see inside the uterus to identify any potential growths.
• Endometrial biopsy: This procedure involves inserting a small, thin tube into the vagina to reach the cervix to take a sample of tissue lining from the uterus. This tissue can then be tested for the presence of abnormal cells, such as cancerous cells.
• Hysteroscopy: This procedure involves a doctor inserting a tool with a thin, lighted camera on the end to examine the inside of the uterus and its lining. The approach can help a doctor to identify polyps or abnormal growths.
• Sonohysterography: This procedure involves injecting fluid through the vagina and into the uterus. A doctor will then use an ultrasound machine – which uses sound waves to identify differences in tissues – to visualize the uterus. This is known as a transabdominal ultrasound. The process can allow a doctor to determine whether the uterine lining is thicker or thinner than expected.
• Transvaginal ultrasound: This procedure involves inserting a special ultrasound probe into the vagina to allow a doctor to visualize the uterus from the bottom of the uterus, instead of from the lower abdomen.
While most of these tests can be performed at a doctor’s office, others, such as a D&C, are often performed at a hospital or surgery center.
Dr. Ruchi Tandon is a Gynecologist practicing in leading hospitals in South Delhi namely Max and Apollo hospitals, with over 14 years of experience in handling all kinds of Gynecological conditions.