About dysmenorrhea
Menstruation occurs when the uterus sheds its lining once a month. Some pain, cramping, and discomfort during menstrual periods is normal. Excessive pain that causes you to miss work or school is not.
Painful menstruation is also called dysmenorrhea. There are two types of dysmenorrhea: primary and secondary.
Primary dysmenorrhea occurs in people who experience pain before and during menstruation. If you’ve had normal periods that become painful later in life, it may be secondary dysmenorrhea. A condition affecting the uterus or other pelvic organs, such as endometriosis or uterine fibroids, can cause this.
What are the causes?
It’s not always possible to identify the cause of painful menstrual periods. Some people are just at a higher risk of having painful periods.
These risks include:
- being under age 20
- having a family history of painful periods
- smoking
- having heavy bleeding with periods
- having irregular periods
- never having had a baby
- reaching puberty before age 11
A hormone called prostaglandin triggers muscle contractions in your uterus that expel the lining. These contractions can cause pain and inflammation. The level of prostaglandin rises right before menstruation begins.
Painful menstrual periods can also be the result of an underlying medical condition, such as:
- Premenstrual syndrome or PMS is a common condition that’s caused by hormonal changes in the body occurring 1 to 2 weeks before menstruation begins. Symptoms typically go away after bleeding begins.
- Endometriosis .This is a painful medical condition in which cells from the lining of the uterus grow in other parts of the body, usually on the fallopian tubes, ovaries, or tissue lining the pelvis.
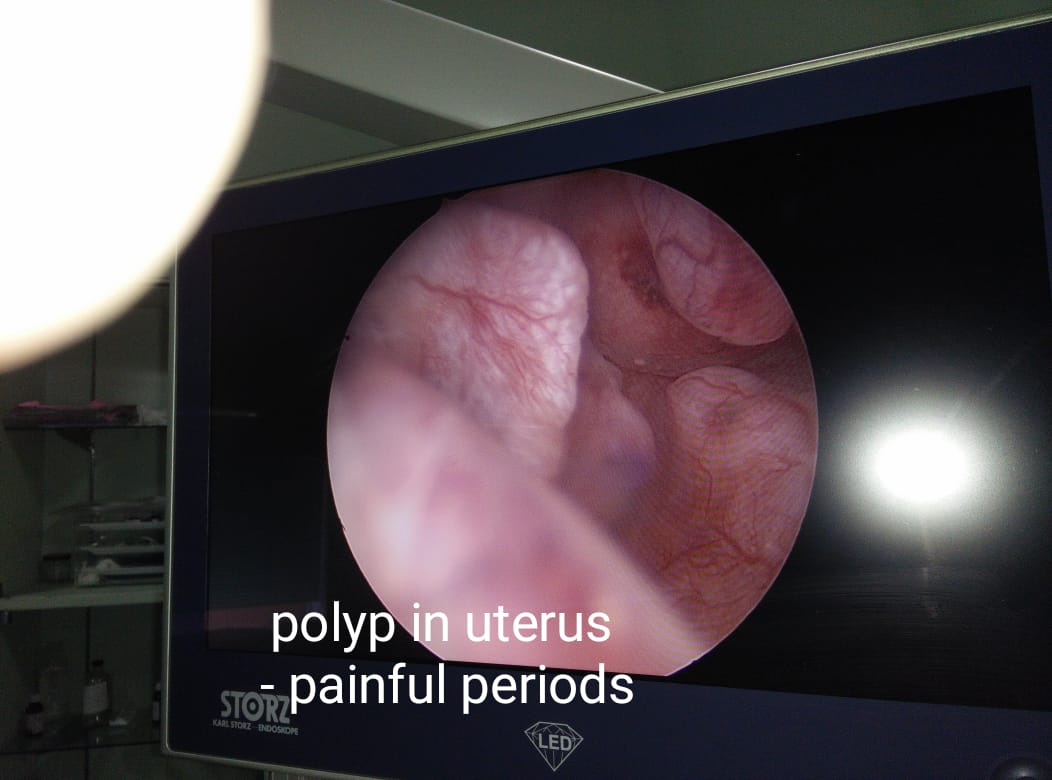
- Fibroids are noncancerous tumors that can put pressure on the uterus or cause abnormal menstruation and pain, though they often don’t cause symptoms.
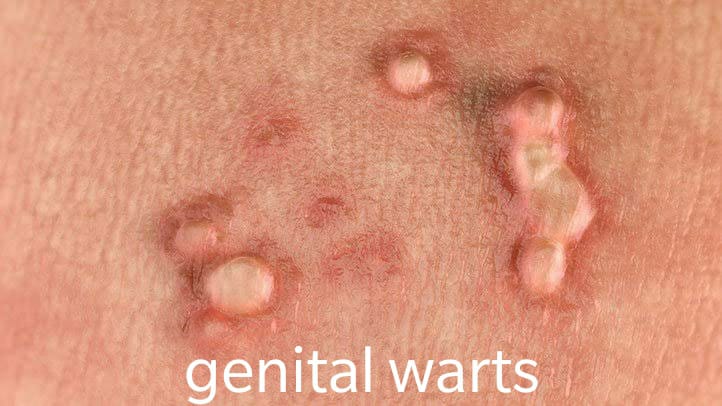
- Pelvic inflammatory disease. PID is an infection of the uterus, fallopian tubes, or ovaries often caused by sexually transmitted bacteria that cause inflammation of the reproductive organs and pain.
- This is a rare condition in which the uterine lining grows into the muscular wall of the uterus, causing inflammation, pressure, and pain. It can also cause longer or heavier periods.
- Cervical stenosis. Cervical stenosis is a rare condition in which the cervix is so small or narrow that it slows menstrual flow, causing an increase of pressure inside the uterus that causes pain.
Home treatment
At-home treatments can be helpful in relieving painful menstrual periods. Types of things to try at home include:
using a heating pad on your pelvic area or back
massaging your abdomen
taking a warm bath
doing regular physical exercise
eating light, nutritious meals
practicing relaxation techniques or yoga
taking anti-inflammatory medications such as ibuprofen several days before you expect your period
taking vitamins and supplements such as:
- Vitamin B6
- Vitamin B1
- Vitamin E
- Omega 3 fatty acid
- Calcium
- Magnesium
- raising your legs or lying with your knees bent
- reducing your intake of salt, alcohol, caffeine, and sugar to prevent bloating
Dr. Ruchi Tandon, is a specialist Gynecologist , practicing in leading hospitals in South Delhi namely Max Smart superspeciality hospital ,saket, Apollo hospitals , with over 13 years experience in handling all kinds of period problems.