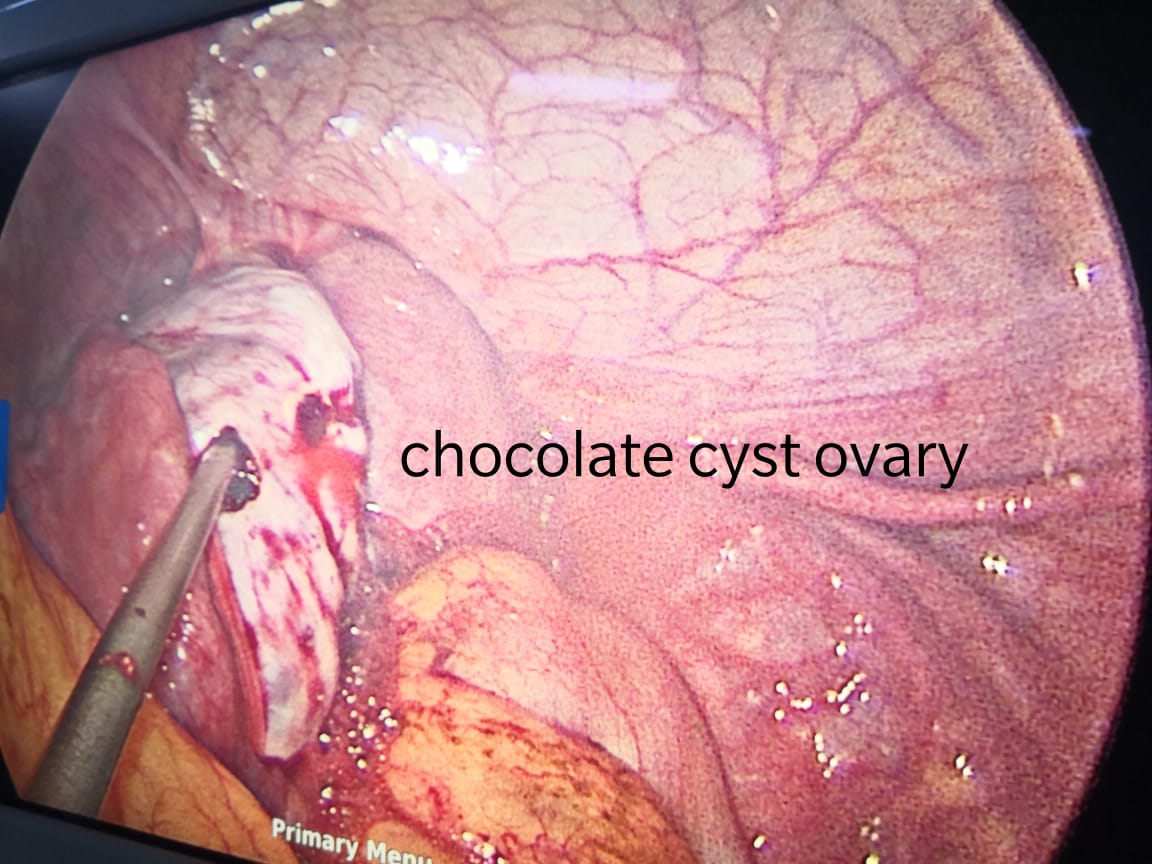
Chocolate cysts are noncancerous, fluid-filled cysts that typically form deep within the ovaries. They get their name from their brown, tar-like appearance, looking something like melted chocolate. They’re also called ovarian endometriomas.
The color comes from old menstrual blood and tissue that fills the cavity of the cyst. A chocolate cyst can affect one or both ovaries, and may occur in multiples or singularly.
Chocolate cysts occur in 20-40 percent of women who have endometriosis, estimates the Endometriosis Foundation of America.
Endometriosis is a common disorder in which the lining of the uterus, known as the endometrium, grows outside the uterus and onto the ovaries, fallopian tubes, and other areas of the reproductive tract. The overgrowth of this lining causes severe pain and sometimes infertility.
Chocolate cysts are a subgroup of endometriosis. They’re often associated with more severe forms of the disorder.
What are the symptoms?
Chocolate cysts may cause symptoms in some women. Other women may not experience any symptoms.
The size of the cyst also doesn’t necessarily affect the severity or presence of symptoms. This means a woman with a small cyst may experience symptoms, while someone with a large one may not. Cysts can range from 2 to 20 centimeters (cm) in size.
When symptoms do occur, they’re similar to those of endometriosis. They can include:
- painful, crampy periods
- Pelvic pain not related to your menstrual cycle
- Irregular periods
- Pain during sex
- infertility for some women
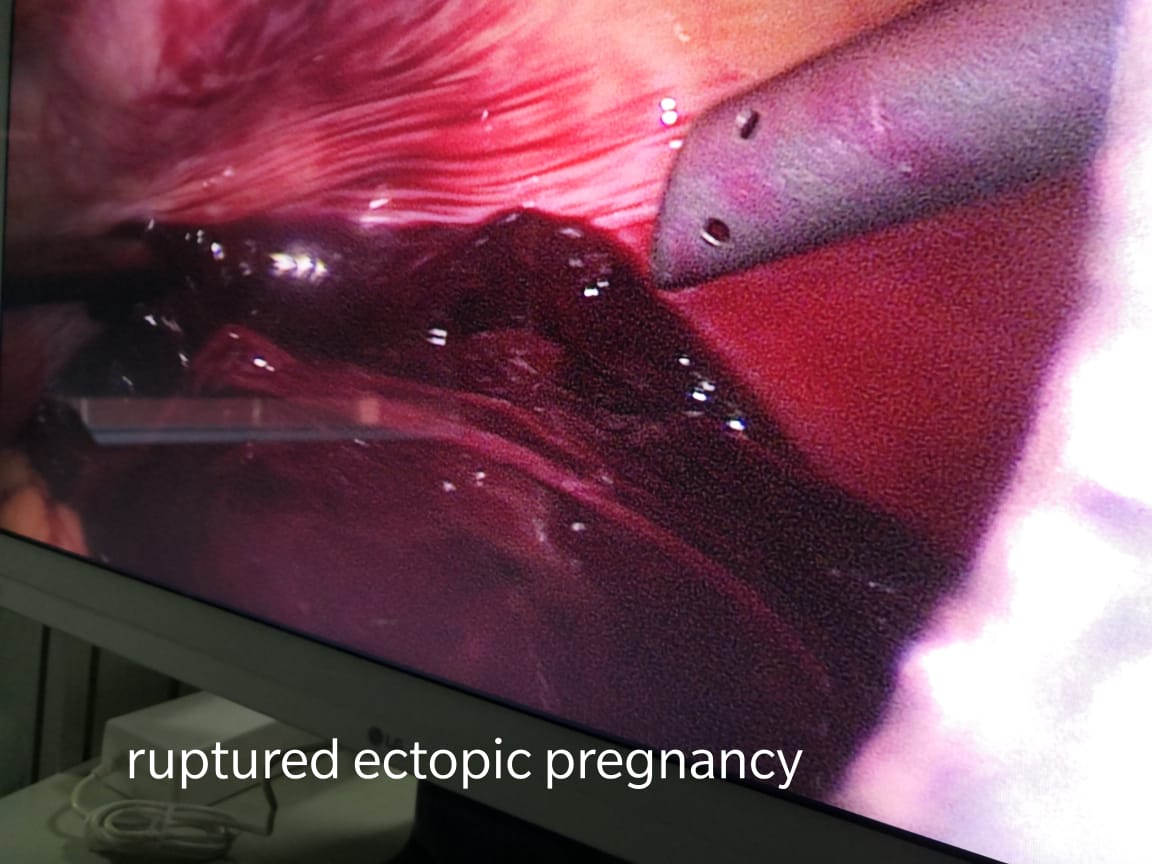
If a chocolate cyst ruptures, it can cause severe, sudden abdominal pain on the side of the body where the cyst is located. A ruptured cyst can be a medical emergency. Seek immediate medical attention if you suspect you have a ruptured cyst.
What causes chocolate cysts?
There’s a lot of debate as to how and why chocolate cysts form. One theory is that they may be a result of endometriosis.
The lining of these cysts acts much the way the lining of the uterus does. It grows and is then shed in response to the monthly rise and fall of female hormones.
Instead of leaving the body, this tissue becomes trapped within the cavity of the cyst. Here it can produce inflammation and disrupt the ovaries.
How are chocolate cysts diagnosed?
Your doctor may order a pelvic ultrasound if:
- they feel a cyst during a pelvic exam
- they suspect you have endometriosis based on your symptoms
- you’re experiencing unexplained infertility
An ultrasound can identify if a cyst is present. But it can’t necessarily determine what type of cyst it is.
To definitively diagnose a chocolate cyst, your doctor will extract fluid and debris from inside the cyst. This is usually done with a needle biopsy.
During a needle biopsy, your doctor will use ultrasound to help them insert a needle through the vagina into the ovarian cyst. The extracted fluid is then examined under a microscope. Your doctor can diagnose the type of cyst using the results from the needle biopsy.
How are chocolate cysts treated?
Treatment will depend on several factors, including:
- your age
- your symptoms
- whether one or both ovaries are affected
- whether or not you want to have children
If the cyst is small and not producing symptoms, your doctor may advise a watch-and-wait approach. They may also recommend medication that inhibits ovulation, such as the birth control pill. This can help control pain and slow the growth of cysts, but it can’t cure them.
Surgery to remove the cysts, called an ovarian cystectomy, is often recommended for women who have:
- painful symptoms
- cysts larger than 4 cm
- cysts that may be cancerous (but a 2006 review estimates less than 1 percent of cysts are cancerous)
- infertility
The surgery is generally done via a laparoscope. A laparoscope is a thin, long tube with a light and camera on the end that helps doctors perform the procedure. It’s inserted through a small incision.
The surgery is controversial in terms of whether it hurts or helps fertility.
Even when the surgeon is highly skilled, healthy ovarian tissue can be removed along with the cyst. That may negatively affect ovarian function. However, the inflammation and toxic environment a chocolate cyst can produce may do more harm to fertility than surgery.
Discuss all of your options and concerns with your Gynecologist before beginning treatment.
Dr. Ruchi Tandon is a Gynecologist practicing in leading hospitals in South Delhi, namely, Max Smart superspeciality hospital, saket, Apollo cradle Royale and is skilled in handling endometriotic or chocolate cysts.