What are uterine fibroids?
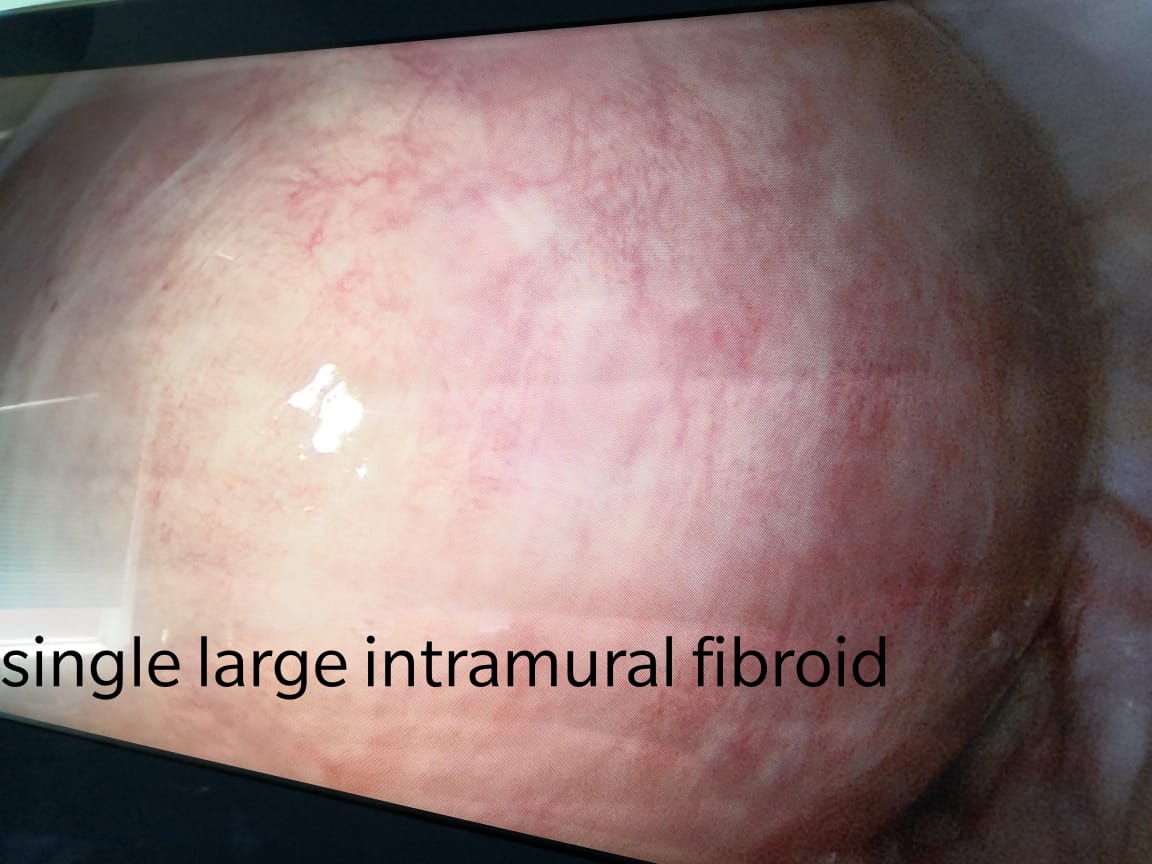
Fibroids are benign tumors made of smooth muscle cells and fibrous connective tissue. They develop in the uterus. It is estimated that 70-80% of women will develop fibroids in their lifetime—however, not everyone will develop symptoms or require treatment. The most important characteristic of fibroids is that they are not cancer, and they do not have the potential to become cancer. Because of that, it is reasonable for women without symptoms to opt for observation rather than treatment. Studies show us that fibroids grow at different rates, even in the same woman, and can range from the size of a pea to the size of a watermelon.
Who is at risk for uterine fibroids?
As women age their likelihood for developing fibroids increases. Studies have demonstrated that women with a family history are more likely to develop fibroids. Fibroids are also more common in African American women. Obesity has also been linked to an increase risk of fibroids. There are no foods or diets that are known to increase a woman’s risk of developing fibroids.
Symptoms
Some women never realize that they have fibroids because they have no symptoms. In other women, uterine fibroids are discovered either during a routine gynecologic exam or during prenatal care.
When symptoms of fibroids occur, they can include:
- Pelvic pain or pressure
- Heavy menstrual bleeding
- Bleeding or spotting between menstrual periods
- Unusually frequent urination
- Abdominal swelling
- Low back pain during intercourse or during menstrual periods
- Fatigue or low energy from heavy periods and excessive bleeding
- Infertility, if the fibroids are blocking the fallopian tubes
- Constipation
- Repeated miscarriages
Diagnosis
Usually, a woman doesn’t realize that she has a fibroid until her gynecologist feels it during a pelvic exam. If your gynecologist thinks you have a fibroid, several tests can confirm the diagnosis:
- Pelvic ultrasound — In this radiology test, a wand-like instrument will be moved over your lower abdomen or may be inserted in your vagina to view the uterus and other pelvic organs more closely. The instrument produces sound waves that create an image of your pelvic organs.
- Hysterosalpingogram— In this X-ray procedure, a dye is injected into your uterus and fallopian tubes to outline any irregularities.
- Hysteroscopy— During this procedure, a narrow instrument that looks like a telescope is inserted through your vagina into your uterus. This lets the doctor look for abnormal growths inside your uterus.
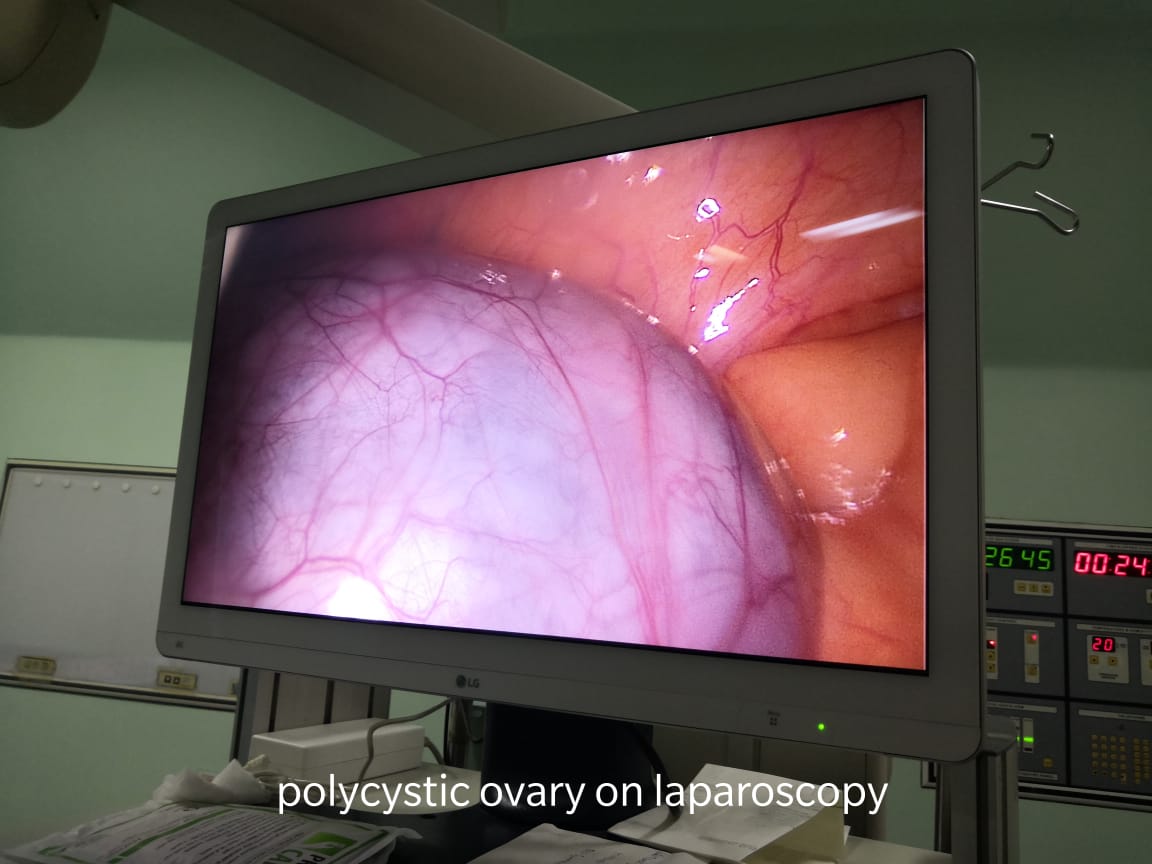
- Laparoscopy— In this procedure, a thin tube-like instrument called a laparoscope is inserted through a small incision in your belly so the doctor can look inside the abdomen.
Expected Duration
The number of fibroids, their size and how fast they grow varies among women. Female hormones encourage fibroids to grow, so they continue growing until menopause. Some fibroids shrink after menopause. However, larger fibroids may change little or become only slightly smaller in size. If a woman has had fibroids removed surgically, new fibroids can appear any time before she enters menopause.
Prevention
There are no proven measures you can take to prevent fibroids from developing. Studies show that athletic women seem to be less likely to develop fibroids than women who are obese or who don’t exercise.
Treatment
If fibroids are small and are not causing any symptoms, they do not need to be treated. Your gynecologist may do a pelvic examination every six months to a year to make sure that your fibroids are not growing rapidly. In some cases, medications can be prescribed to control any abnormal bleeding and temporarily shrink the fibroids.
Medications used to shrink fibroids, such as leuprolide (Lupron), create a temporary menopause by stopping the ovaries from making the female hormone estrogen. While estrogen levels drop and menstrual periods stop, menopausal hot flashes appear and fibroids stop growing and slowly shrink. This helps to stop blood loss from heavy, prolonged periods. However, when the medication is stopped periods return, hot flashes disappear and fibroids that have not been removed will start growing again. These medications usually are given by needle injection in a large muscle.
Fibroids may need to be removed if they cause significant symptoms or are large enough to interfere with fertility. Growths in your uterus also may need to be removed if it is difficult for your doctor to tell whether they are fibroids or cancer. There are several options for removing fibroids:
- Myomectomy— This means cutting the fibroids from the uterine wall. Myomectomy allows a woman to keep her entire uterus in case she wants to have children. However, because this surgery can leave the uterine wall weakened, future babies may have to be delivered by Caesarean section. Surgery to remove fibroids sometimes can be done by laparoscopy, which is surgery through several small incisions in the lower abdomen. When fibroids are too large or too abundant to perform a laparoscopic procedure, then a traditional approach through a larger incision in the lower abdomen is preferred.
- Hysteroscopic resection — In this procedure, a viewing instrument called a hysteroscope is inserted into the uterus through the vagina. Surgical instruments attached to the hysteroscope are used to remove fibroids growing inside the uterus. This procedure sometimes is done in combination with laparoscopy, depending on the number and location of the fibroids.
- Uterine artery embolization — In this X-ray-guided procedure, material is injected into specific blood vessels to plug them and stop blood flow to a fibroid or fibroids. It is an option for a woman who may not be medically cleared for surgery or who does not plan to have more children, but prefers not to have her uterus removed.
- Hysterectomy — In this procedure the uterus is removed including all fibroids within it. Though other options are available to treat or remove fibroids and the patient’s needs and goals must be fully considered, in some cases hysterectomy is the preferred treatment. This may include situations in which fibroids are too numerous, too large, or cause heavy prolonged bleeding and severe anemia. Some patients may prefer hysterectomy so they can be assured the fibroids will not grow back.
Dr.Ruchi Tandon is a Gynecologist with over 13 years of clinical experience in handling fibroids. At present, she is available at all leading South Delhi hospitals.