Uterine fibroids are tumors that grow in a woman’s womb (uterus). These growths are typically not cancerous (benign)
Causes
Uterine fibroids are common. As many as one in five women may have fibroids during their childbearing years. Half of all women have fibroids by age 50.
Fibroids are rare in women under age 20. They are more common in African Americans than White, Hispanic, or Asian women.
No one knows exactly what causes fibroids. They are thought to be caused by:
• Hormones in the body
• Genes (may run in families)
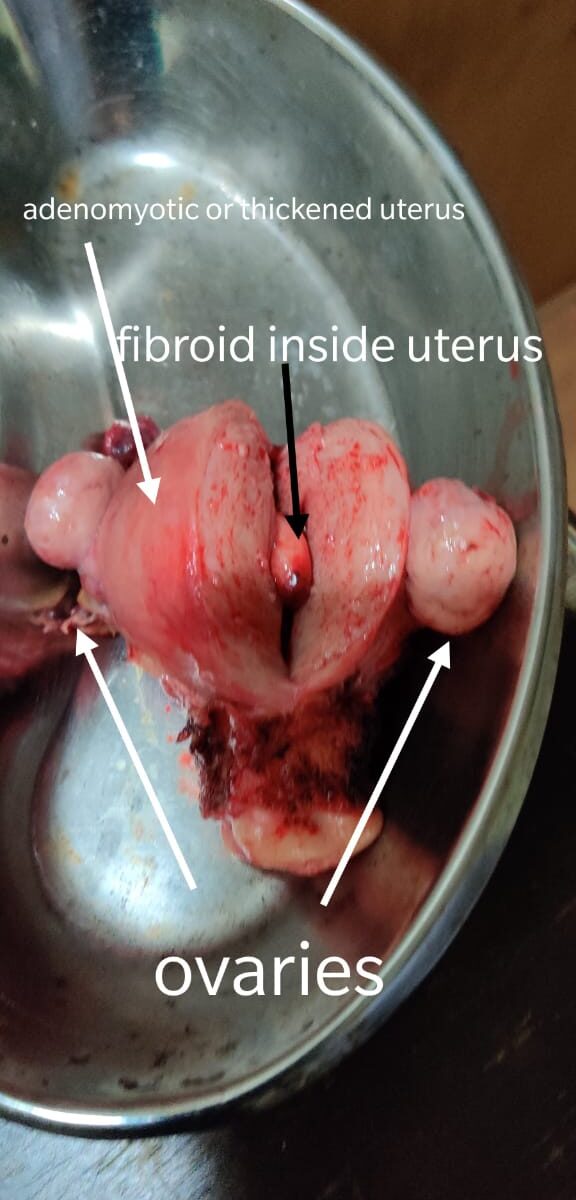
Fibroids can be so tiny that you need a microscope to see them. They can also grow very large. They may fill the entire uterus and may weigh several pounds or kilograms. Although it is possible for just one fibroid to develop, most often there is more than one.
Fibroids can grow:
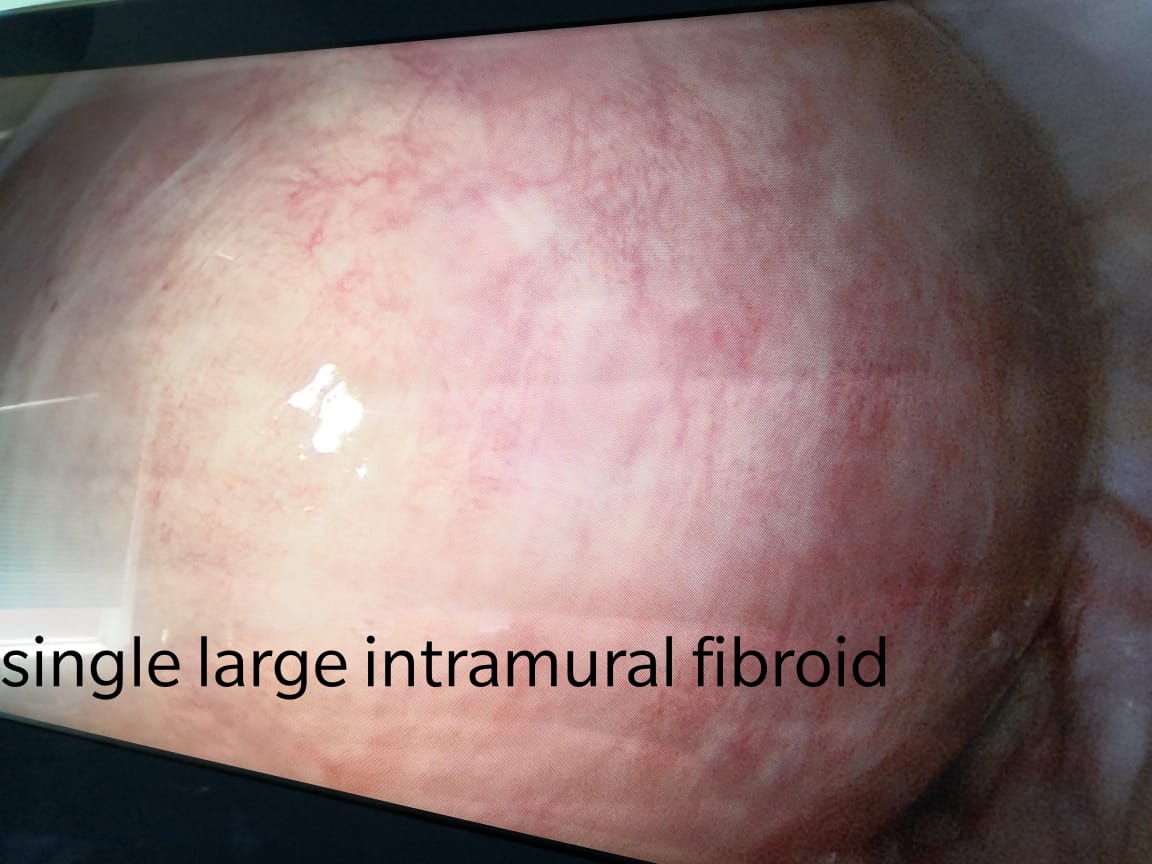
• In the muscle wall of the uterus (myometrial)
• Just under the surface of the uterine lining (submucosal)
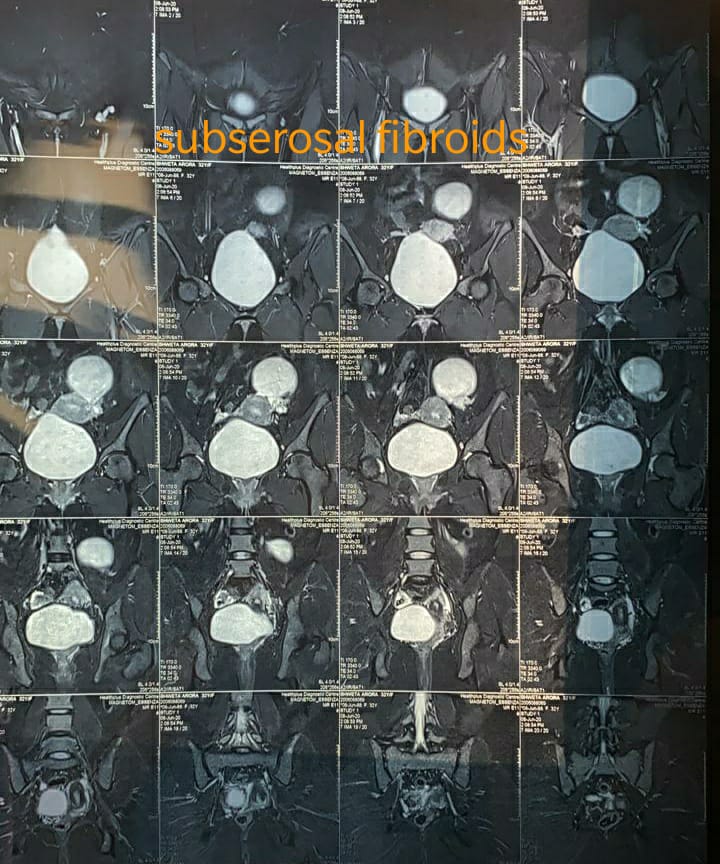
• Just under the outside lining of the uterus (subserosal)
• On a long stalk on the outside the uterus or inside the uterus (pedunculated)
Symptoms
Common symptoms of uterine fibroids are:
• Bleeding between periods
• Heavy bleeding during your period, sometimes with blood clots
• Periods that may last longer than normal
• Needing to urinate more often
• Pelvic cramping or pain with periods
• Feeling fullness or pressure in your lower belly
• Pain during intercourse
Often, you can have fibroids and not have any symptoms. Your health care provider may find them during a physical exam or other test. Fibroids often shrink and cause no symptoms in women who have gone through menopause. A recent study also showed that some small fibroids shrink in premenopausal women.
Evaluating Uterine Fibroid Size for Removal
Women with large or symptom-producing fibroids may need to have an imaging study done to evaluate uterine fibroid size to determine whether it needs to be removed. The risk of not getting treatment is that fibroids sometimes grow to a size that often leads to significant symptoms, eventually requiring removal.
Larger fibroids or those that continue to grow may lead to complications.
• If submucosal fibroids are found on the inside of the uterus and are large enough to misshape the uterine lining, they should be removed to prevent reproductive problems. (iii)
• If fibroids are larger than a 12- to 14-week pregnancy (about the size of a large grapefruit), the risk of complications during surgery, such as injury to the ureter or bladder, increases. (i)
• Left untreated, very large fibroids can begin to degenerate or burst, even if they aren’t causing any symptoms. (i) Degeneration occurs when the growing fibroid outgrows its blood supply, causing the cells of the fibroid to die. This typically causes abrupt, severe pain and tenderness.
• When fibroids reach the size of a grapefruit (4 – 6 inches), there is a rare association with blood clots in the lungs, which can be deadly. (i)
• Rapidly growing large fibroids may be a sign of a rare cancerous form of fibroid, called a leiomyosarcoma. This type of tumor can’t be differentiated from a non-cancerous (benign) fibroid using ultrasound, MRI, or other imaging studies. However, this type of fibroid only occurs in less than 1percent of uterine fibroids, and these cancerous tumors are not believed to grow from a benign fibroid. (ii)
Treatment Options for Uterine Fibroids
There are several uterine fibroid treatment options:
• Uterine fibroid embolization (UFE) uses tiny particles about the size of sugar crystals that are injected into the blood vessels that lead to the uterus. The particles block the flow of blood to the fibroid, causing it to shrink and die. This minimally invasive procedure can be performed by an interventional radiologist on an outpatient basis. It doesn’t require open surgery and offers relief of symptoms with fewer risks, less pain, and a faster recovery compared to surgical procedures.
• Magnetic resonance imaging-guided (MRI) ultrasound surgery uses ultrasound waves to destroy fibroids. Waves are directed at the fibroids through the skin with the help of magnetic resonance imaging.
• Endometrial ablation destroys the lining of the uterus. This procedure is best for small fibroids that are less than 3 centimeters in diameter. (v)
• Hysterectomy is the surgical removal of the uterus. Because this surgery removes the fibroids along with the uterus, there is no chance of becoming pregnant after undergoing a hysterectomy.
• Myomectomy is another surgical option to remove all types of fibroids. There are three approaches to performing a myomectomy: hysteroscopy, laparotomy, and laparoscopy.
How large do uterine fibroids need to be before being surgically removed?
The normal uterine size is the size of a lemon or 8 cm. There isn’t a definitive size of a fibroid that would automatically mandate removal. Your healthcare provider will determine the symptoms that are causing the problem. Fibroids the size of a marble for instance, if located within the uterine cavity, may be associated with profound bleeding. Fibroids the size of a grapefruit or larger may cause you to experience pelvic pressure, as well as make you look pregnant and see increased abdominal growth that can make the abdomen enlarged.
It’s important for the healthcare provider and patient to discuss symptoms which might require surgical intervention.
Dr. Ruchi Tandon is a Gynecologist practicing in leading hospitals in South Delhi namely Max and Apollo hospitals with over 14 years of experience in handling all kinds of Gynecological conditions including Fibroids. She is one of the best fibroids surgeon in south delhi.