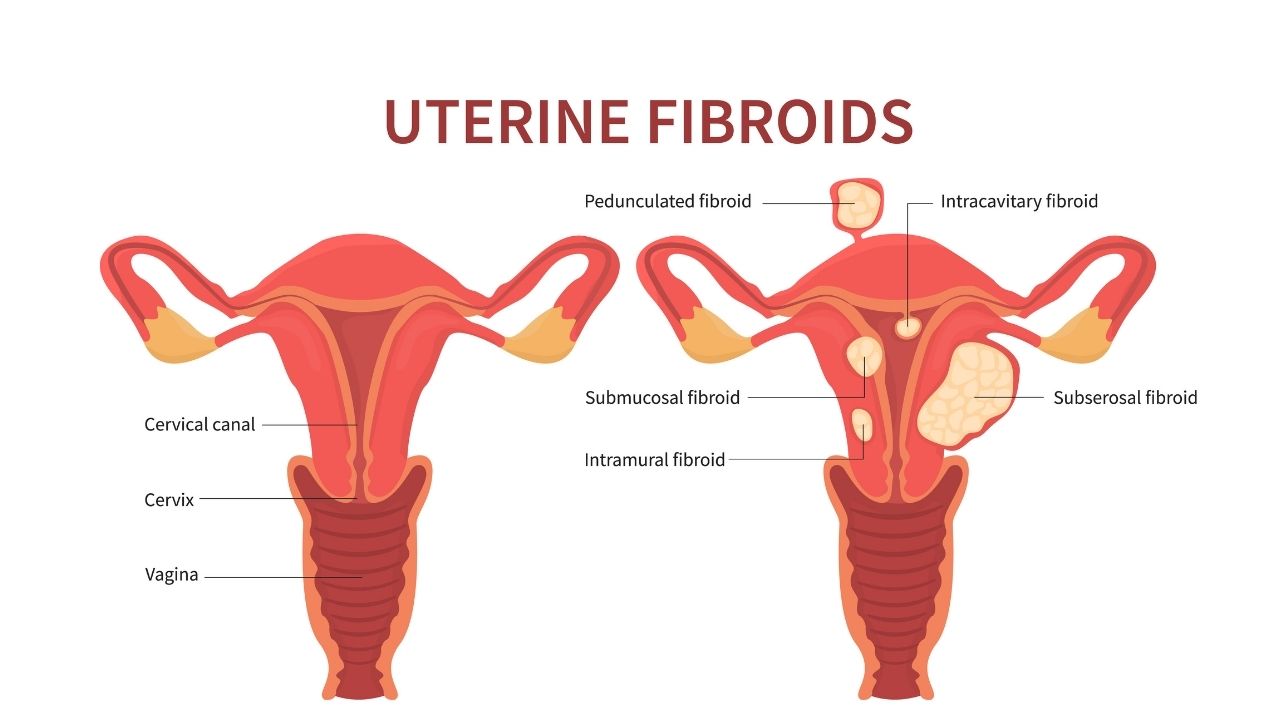
Uterine fibroids are noncancerous growths that grow in the wall of the uterus. When fibroids cause heavy bleeding or painful symptoms, and other treatments are ineffective, a doctor may recommend surgery.
Fibroids are common, but it is challenging for doctors to determine what percentage of people have them, as not everyone experiences symptoms. According to various estimates, fibroids may affect between 20% and 80% of the female population under the age of 50 years.
Although fibroids can sometimes grow to the size of a grapefruit or even larger, they are often very small. Many people with fibroids are unaware that they have them. People with asymptomatic fibroids do not require surgery or other treatments.
However, other people experience abdominal pain, pressure, bloating, pain during sex, frequent urination, and heavy or painful periods. These individuals may require surgery.
In this article, learn more about surgery for fibroids, including the types, risks, and what to expect.
There are several different surgical approaches to treating fibroids. The types of surgery that a person can have will depend on the location of the fibroid.
A doctor will usually recommend more conservative options, such as medication, before considering surgery.
In cases where medication and other treatments do not work, surgical options include the following:
Myomectomy
Myomectomy is a surgical procedure that removes fibroids. Depending on the location of these growths, a surgeon may also have to remove other tissue in the process. Surgeons offer different myomectomy techniques.
The traditional technique is quite invasive as it uses a relatively large cut. This incision may go from the bellybutton to the bikini line or run horizontally along the bikini line. Some surgeons also perform laparoscopic surgeries, which use smaller incisions but require more skill.
Although a myomectomy preserves the uterus, women who wish to become pregnant should speak to a doctor about the possible complications. Those with very large or deeply embedded fibroids may only be able to have cesarean deliveries after this procedure.
New fibroids may develop after a myomectomy, which means that it is not a permanent solution for everyone.
Radiofrequency ablation procedure
Radiofrequency ablation destroys fibroids using either an electric current, a laser, cold therapy, or ultrasound. It requires only a small incision.
However, it can cause dangerous pregnancy complications, such as scarring and infection, so doctors do not recommend it for those who are planning future pregnancies.
Radiofrequency ablation may be a good option for people considering a hysterectomy who want a less invasive procedure.
Endometrial ablation
Endometrial ablation does not remove fibroids, but it can help relieve heavy bleeding.
During endometrial ablation, a surgeon uses a range of techniques — which may include heat, electric current, freezing, lasers, or wire — to destroy the lining of the uterus. These techniques reduce or stop heavy bleeding.
This procedure is less invasive than some other surgical options. Sometimes, doctors can even perform it on an outpatient basis in their office.
This procedure may prevent women from being able to get pregnant in the future, so it is not a good option for those who would still like to have children.
Hysterectomy
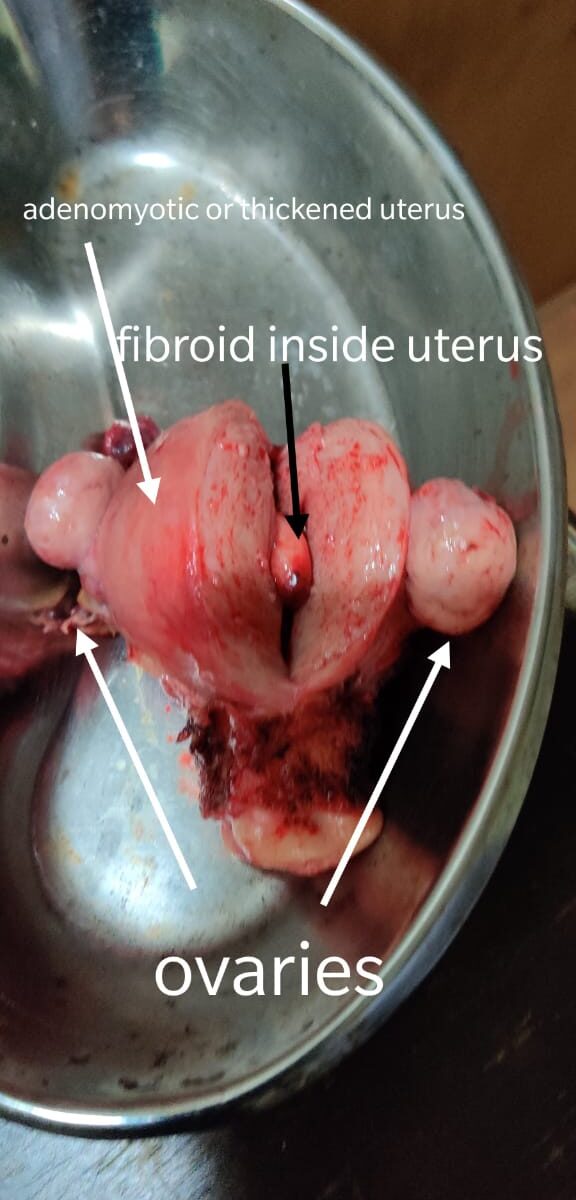
A hysterectomy is a surgery to remove the uterus and, sometimes, the ovaries. A hysterectomy permanently eliminates uterine fibroids.
This procedure is not an option for anyone planning a future pregnancy, as it removes the womb. Some people opt to leave the ovaries in place so that they continue producing estrogen.
A surgeon may be able to perform a laparoscopic hysterectomy, which uses several small incisions and a tiny camera to help the surgeon see inside the abdomen. An open hysterectomy requires a large incision between the bellybutton and the bikini line.
Another option is a vaginal hysterectomy, which is the approach that most people prefer. In this procedure, a surgeon will remove the uterus through the vagina.
A vaginal hysterectomy may not be possible if the uterus or fibroid is too large to fit through the vagina.
Individuals who undergo an open hysterectomy may have a longer recovery time. Doctors usually recommend a hysterectomy only for those whose fibroids are very large or significantly interfere with their quality of life.
People who have other reproductive health issues, such as endometriosis, may find that a hysterectomy provides significant relief from fibroids and other symptoms.
Morcellation
Morcellation is a procedure that reduces the size of fibroids so that a surgeon can remove them through a tiny incision in the abdomen. A doctor may use morcellation during a myomectomy, hysterectomy, or other surgery.
However, the Food and Drug Administration (FDA) caution that morcellation carries significant risks.
While fibroids are not cancerous, uterine cancer is more common in people having fibroid surgery than experts previously thought.
It can also be difficult to tell the difference between a fibroid and a type of cancer that looks the same. According to the FDA, morcellation may inadvertently spread cancer that resembles a fibroid.
Benefits
The benefits of surgery depend on the type of surgery and can vary from person to person. For example, there is no chance that the fibroids will grow back after a hysterectomy. However, they may regrow following other procedures.
Some potential benefits include:
• reduced bleeding
• relief from pain or pressure
• removal of fibroids
• the potential that fibroids will either not grow as large or not regrow at all
Dr. Ruchi Tandon is a reputed Gynecologist practicing in leading hospitals in South Delhi namely Max and Apollo hospitals with over 13 years experience in handling all kinds of fibroids.